Birth asphyxia occurs when a baby’s brain is deprived of oxygen shortly before, during, or after birth. This may be due to an interruption in the transportation of oxygenated blood from a mother to her unborn baby, an issue with blood circulation within the baby’s body, or (if it happens after birth) an airway blockage.
Birth asphyxia often causes hypoxic-ischemic encephalopathy (HIE), a form of neonatal brain damage that can lead to cerebral palsy (CP), epilepsy, and other disabilities. If a baby has HIE, they should be given therapeutic hypothermia very shortly after the birth asphyxia occurs; this can minimize the extent of permanent brain damage.
Because birth asphyxia, HIE, and resultant disabilities are often preventable, parents may choose to pursue a birth injury lawsuit. The attorneys at ABC Law Centers may be able to help.
Relevant terminology
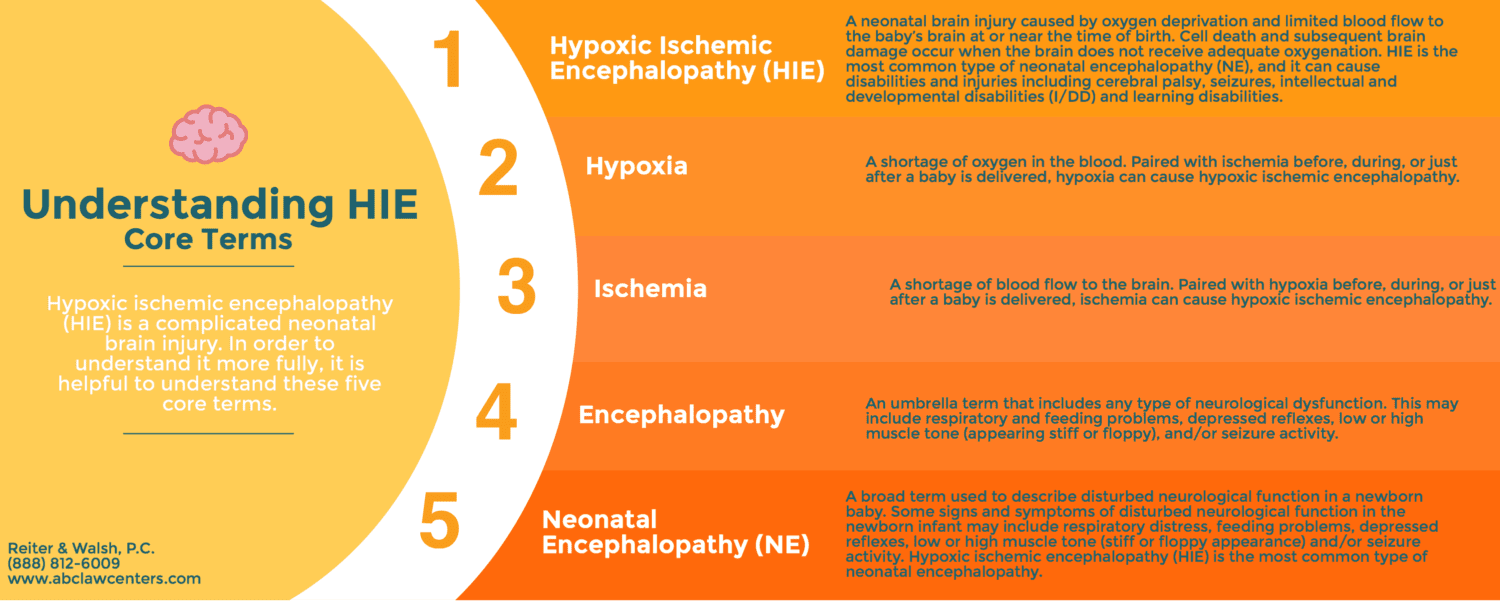
Terms which are sometimes used as synonyms for birth asphyxia include neonatal asphyxia, perinatal asphyxia, intrapartum asphyxia, neonatal encephalopathy, and hypoxic-ischemic encephalopathy; however, each term has its own unique meaning.
What causes birth asphyxia?
Inside the womb, oxygen-rich blood from the mother travels from the uterus through the placenta and umbilical cord in order to reach the baby. Blood vessels that run between the uterus and placenta, called the uteroplacental circulation, act in a manner similar to the lungs; gas exchange takes place in these vessels.
Anything that affects blood flow along this pathway can impact the baby’s oxygenation. Thus, if the mother’s blood pressure drops or there are problems with the uterus (womb), placenta, or umbilical cord, the baby may experience birth asphyxia. In certain cases, such as a complete placental abruption or umbilical cord compression, the baby can be completely deprived of oxygen-rich blood and will then have to rely on fetal reserves. Instances such as these are obstetrical emergencies and the baby must be delivered right away before birth asphyxia causes brain damage.

Common causes and risk factors for birth asphyxia include:
- Umbilical cord problems, including the following:
- Placental complications, including the following:
- Uterine hyperstimulation/tachysystole (this may be caused by the improper use of labor-enhancing drugs such as Pitocin and Cytotec)
- Preeclampsia/eclampsia
- Anesthesia mistakes, which can cause blood pressure problems in the mother, including a hypotensive crisis. This can greatly decrease the supply of oxygen-rich blood going to the baby.
- Oligohydramnios (low amniotic fluid)
- Premature rupture of the membranes (PROM)
- Premature birth
- Prolonged and arrested labor
- Postmaturity syndrome
- Failure to quickly deliver a baby when signs of fetal distress are evident on the fetal heart rate monitor (delayed emergency C-section)
The short-term effects of birth asphyxia
Birth asphyxia occurs when gas exchange between the mother and fetus is impaired. A condition known as hypoxia is an early stage of birth asphyxia. Hypoxia is characterized by insufficient oxygen levels in the blood and tissues. Carbon dioxide levels in the fetus will also increase, which is known as hypercarbia. When severe hypoxia occurs, the fetus begins to generate energy without oxygen, in a process known as anaerobic metabolism. This process causes lactic acid to build up in the baby’s blood (1). Birth asphyxia can also cause the baby to have acidosis, a process by which the blood becomes acidic (2). Acidosis and hypoxia can cause decreased heart function, which can cause the baby to have very low blood pressure (hypotension) and decreased blood flow to the brain (ischemia).
Ischemia can then cause further hypoxia, essentially creating a vicious cycle. Hypoxia and ischemia cause a series of events that disrupt the energy pathways in the cells, which can worsen existing brain cell injury. When the brain is in a hypoxic-ischemic state caused by prolonged birth asphyxia, the brain is not only deprived of oxygen, it is also deprived of glucose and other nutrients.
In general, the longer the brain is in a hypoxic-ischemic state, the more severe the brain injury will be (1).
The degree of hypoxic-ischemic brain injury in the baby depends on the following:
- The severity of the birth asphyxia
- How long the birth asphyxia lasts
- The baby’s age and reserves
- The medical management of the baby during and after birth
Long-term impacts of birth asphyxia: the side effects of hypoxic-ischemic encephalopathy (HIE)
If the birth asphyxia is severe enough to injure the brain, the baby will usually develop hypoxic-ischemic encephalopathy (HIE) soon after birth. HIE is a brain injury that can progress to permanent brain damage and long-term conditions, such as cerebral palsy.
Clinical signs of HIE in babies:
- Neonatal seizures
- Hypotonia, in which the baby is limp and floppy.
- Poor feeding
- Depressed level of consciousness, in which the baby is not alert.
- Multiple organ problems involving the lungs, liver, heart, intestines, etc.
- Poor brain stem reflexes such as breathing problems, an abnormal response to light, blood pressure and heart problems.
Hypoxic-ischemic encephalopathy is the most common cause of neonatal seizures (3). Seizures must be quickly diagnosed and treated because they can advance the spread of brain injury. It is also very important that the medical team be aware of any other problems the baby is having, so that they can provide proper treatment. For example, babies experiencing heart problems often require cardiac drugs. Babies with breathing problems may need breathing tubes and breathing machines. Failure to properly manage a baby’s heart, blood pressure, and breathing can cause further brain injury and worsen the long-term effects of birth asphyxia.
Premature babies may not show any of the signs that full-term babies do. One reason for this is the fact that the nervous systems of premature and full-term babies are different. Hypoxic-ischemic brain injury in a baby born preterm may be silent, with the baby having few or no obvious signs.
In term babies, HIE usually involves damage to the basal ganglia and watershed regions of the brain. However, there can also be other patterns of injury. For example, premature babies often have periventricular leukomalacia (PVL) (4).
Treatment: therapeutic hypothermia can halt HIE and minimize the long-term effects of birth asphyxia

It is now the standard of care for babies diagnosed with HIE to receive therapeutic hypothermia (brain cooling). Most guidelines dictate that doctors must administer hypothermia therapy within six hours of the time the birth asphyxia occurred. Generally, this means a baby with HIE must be cooled within six hours of birth.
Research shows that therapeutic hypothermia slows almost every injurious process that starts to occur when a baby’s brain experiences birth asphyxia. During the treatment, the baby’s body temperature is cooled to a few degrees below normal for 72 hours. Cooling the brain in this way has been shown to prevent cerebral palsy or reduce the severity of the condition. Properly administering hypothermia treatment on a baby with HIE is critical for preventing or improving the long-term effects of birth asphyxia.

For more information on therapeutic hypothermia, please visit our pages below:
- Hypothermia Therapy Errors
- Eligibility Criteria for Hypothermia Therapy
- Hypothermia Therapy May Be Effective 6-24 Hours After Birth: The study discussed here was statistically inconclusive, but warrants further research on the window of time in which hypothermia therapy can be effective.
Long-term effects of birth asphyxia
Many babies who experience birth asphyxia are diagnosed with hypoxic-ischemic encephalopathy shortly after birth. Not all children with HIE end up with permanent brain damage. Some children will not experience any long-term effects of birth asphyxia or any latent problems from HIE. However, babies who have brain damage caused by birth asphyxia or HIE may develop the following conditions:
- Cerebral palsy and other motor disorders
- Epilepsy and seizure disorders
- Developmental delays
- Speech delays
- Learning disabilities
- Behavioral and emotional disorders
- Hearing impairments
- Visual impairments
- Feeding problems, nutritional concerns, and oral health issues
- Pain symptoms
- Respiratory conditions
- Skin issues
- Orthopedic issues
- Mental health conditions
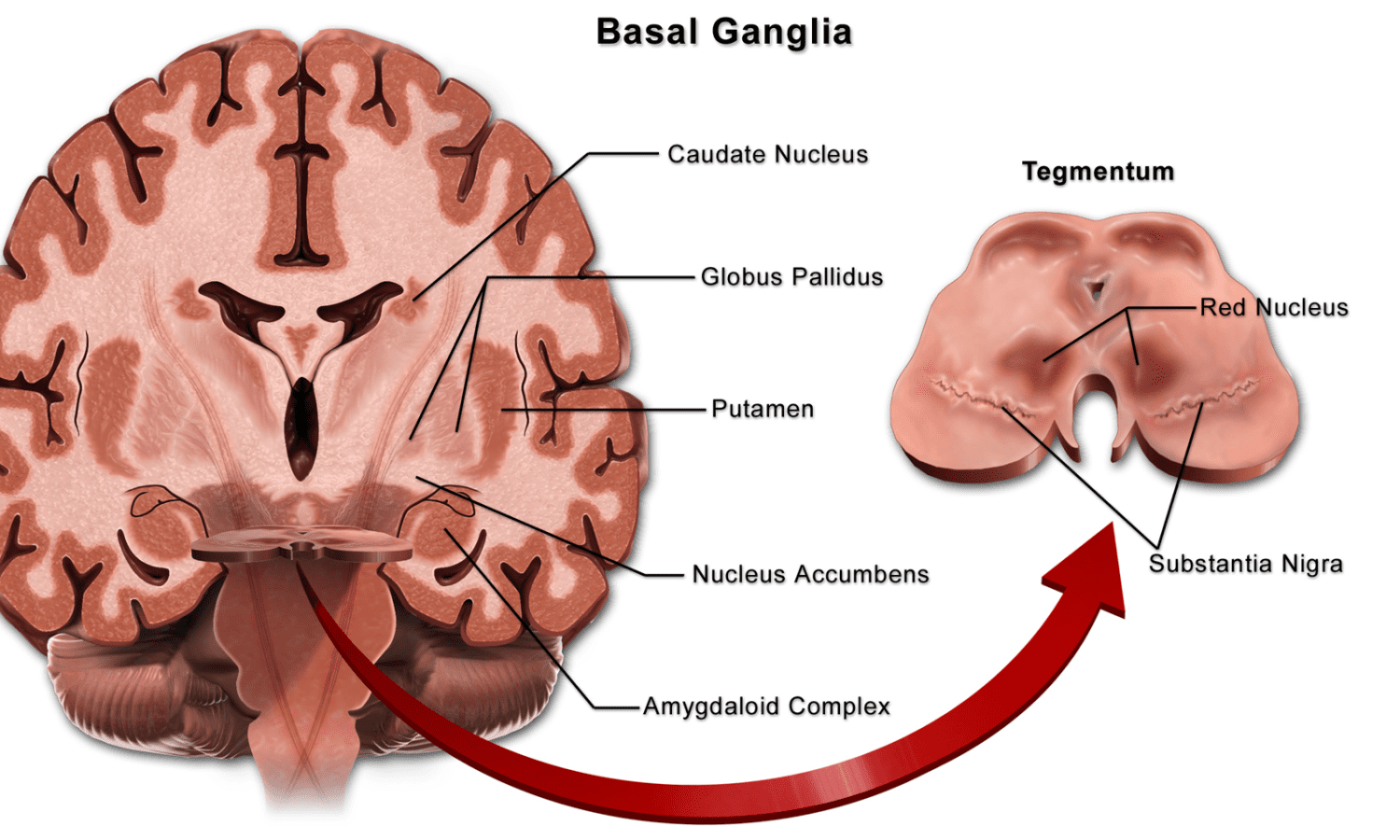
The long-term effects of birth asphyxia depend on the part of the brain injured and the severity of the injury. In late preterm and term infants, there are two common patterns of injury (5):
- When an infant experiences “acute profound” or “acute near total” asphyxia, there is typically damage to the deep gray matter of the brain (5). This may include the basal ganglia, thalamus, and brain stem (6).
- When an infant experiences partial prolonged asphyxia, there is more likely to be parasagittal injury in the cerebral cortex and subcortical white matter. This may be described as a “watershed” pattern of injury (5).
Babies can also experience partial prolonged asphyxia along with acute profound asphyxia, which causes a “mixed brain injury pattern” of HIE.
When a baby has hypoxic-ischemic encephalopathy, brain lesions are often detected with brain scans. Depending on the nature of the birth asphyxia and the condition of the baby, lesions may be on any part of the brain mentioned above (and others).
Predicting the long-term effects of birth asphyxia based on location of brain damage
The extent and location of the brain damage can help doctors predict the long-term effects of birth asphyxia, as well as what types of lasting problems the child may have. Listed below are areas of the brain that may be injured, and summaries of which bodily functions these areas help control. The three major parts of the brain are the cerebrum, cerebellum, and brain stem, all of which contain both gray and white matter.
The cerebrum
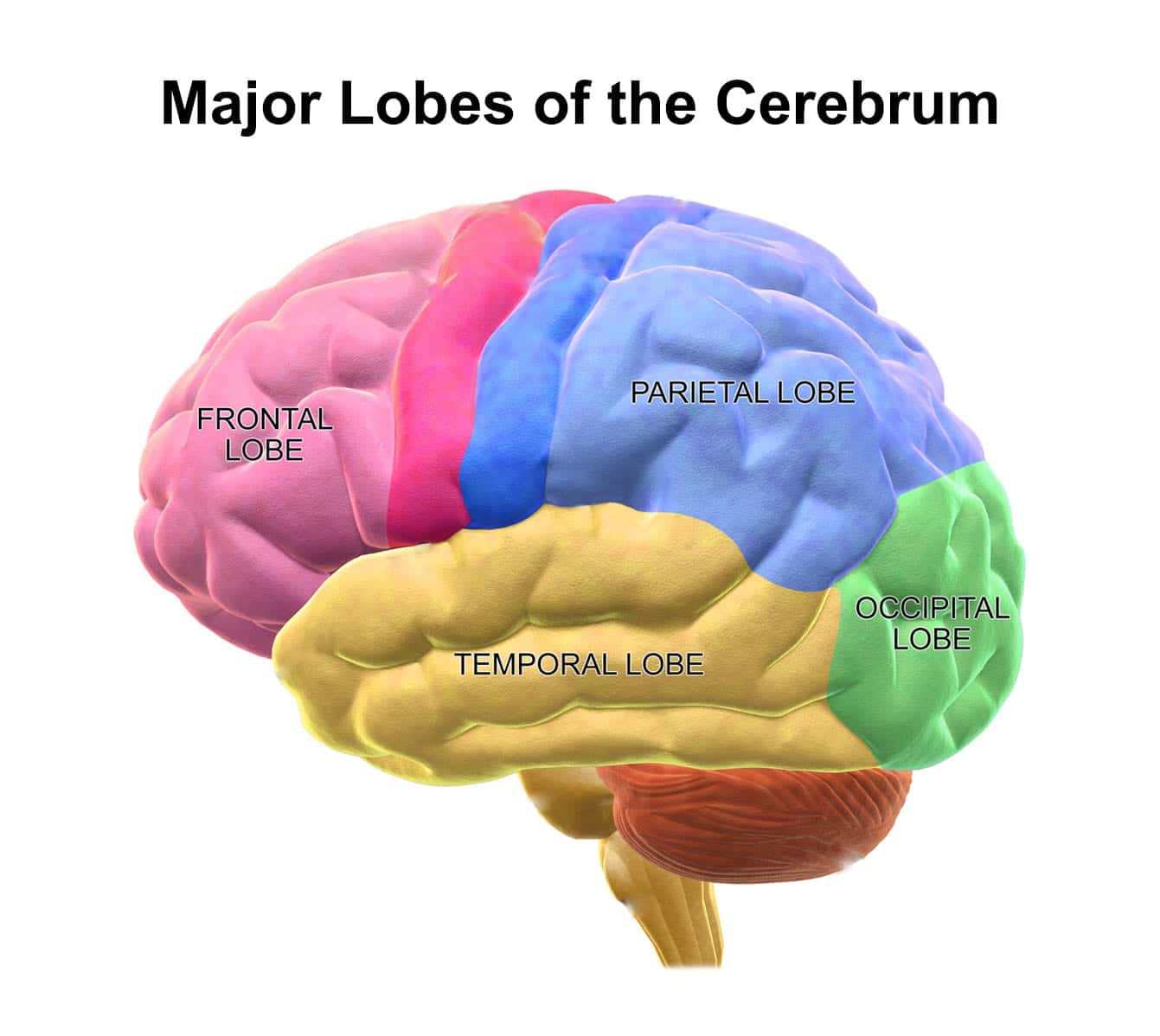
The largest part of the brain, the cerebrum, contains nerve centers that control movement, reasoning, memory, perception, and judgment (7). The surface of the cerebrum is called the cerebral cortex, which helps to coordinate motor and sensory information (8). The cerebrum has four lobes, each of which plays an important role in brain function.
Frontal lobes of the cerebrum
The frontal lobes play a critical role in high-level functions such as movement, attention, planning, and judgment. These lobes also manage emotions and impulse control, and greatly influence individual personality.
Parietal lobes of the cerebrum
The parietal lobes are behind the frontal lobes. They work to organize and interpret sensory information that is sent from other brain regions.
Temporal lobe of the cerebrum
These lobes are located near the ears. They have an important role in functions such as language comprehension, visual memory (i.e. facial recognition), and understanding emotions (7).
Occipital lobe of the cerebrum
The occipital lobe is at the back of the head and contains the primary visual cortex, which controls vision. The occipital lobe is very important in both receiving and processing visual information. For example, it is involved in reading and reading comprehension (9).
The cerebellum
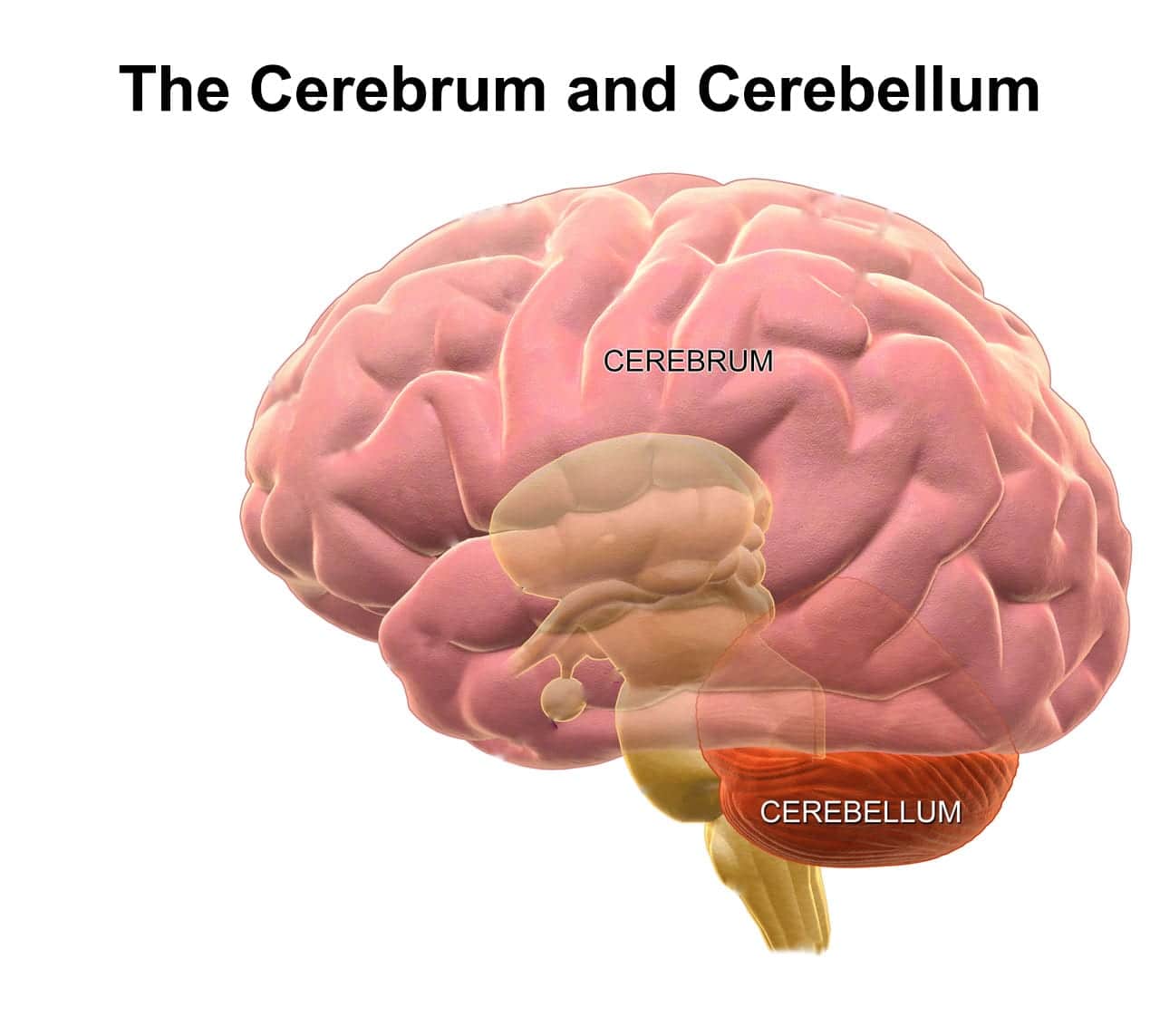
The cerebellum is just behind the top of the brain stem, where the brain connects with the spinal cord. Although the cerebellum is approximately 10 percent of the brain’s total weight, it contains about half of the brain’s neurons.
The cerebellum plays a major role in motor control (voluntary movement). When the cerebellum functions normally, muscle movements will be smooth and the person will have good posture, balance, coordination, and speech. Although damage to the cerebellum would not result in paralysis, it can cause balance problems, inefficient movement, tremors, and other motor control issues. This type of brain damage also makes it harder for children to learn new motor tasks (10).
The brain stem
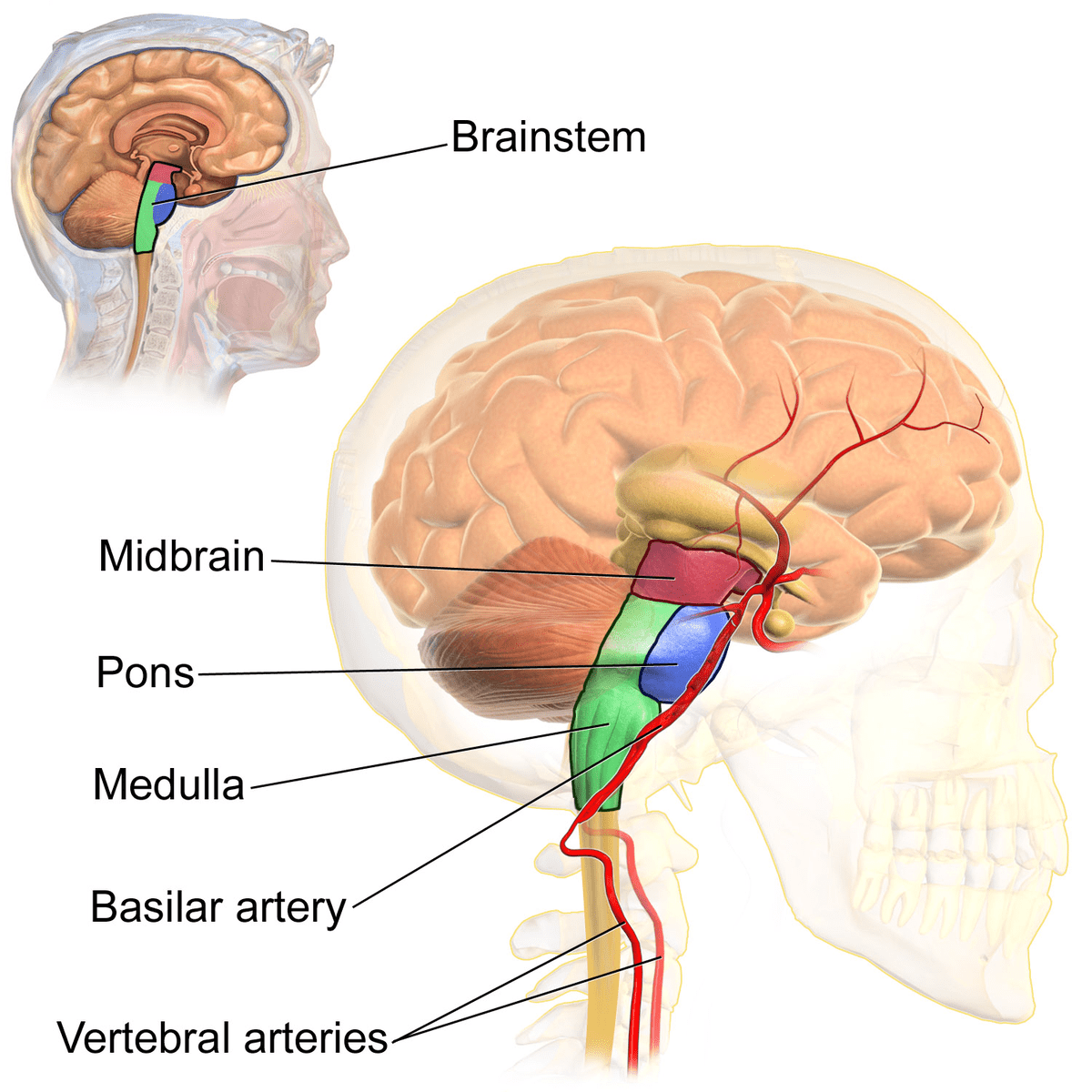
The brainstem is positioned in front of the cerebellum, and relays signals from the brain to the spinal cord. It helps regulate bodily functions such as breathing, heart rate, and blood pressure, and is critical to survival (11). The brainstem consists of three major parts: the pons, midbrain, and medulla oblongata.
Pons
The pons is the largest part of the brain stem. It is involved in the transmission of sensory information. It also controls facial movements.
Midbrain
The midbrain helps process both visual and auditory information. It also plays a role in controlling eye movement.
Medulla oblongata
The medulla oblongata is what connects the brainstem to the rest of the brain. It controls the heart and lungs, and regulates important functions such as breathing and swallowing (7).
Detroit, Michigan attorneys helping children with birth asphyxia

Cases involving birth asphyxia and hypoxic-ischemic encephalopathy require extensive knowledge of both law and medicine. ABC Law Centers was established to exclusively handle birth injury cases, and our attorneys have the expertise necessary to win. Our firm is based near Detroit, Michigan, but we handle cases in many parts of the country.
Contact ABC Law Centers today to learn more. We are happy to speak with you even if you are not yet sure whether malpractice occurred or if you would like to pursue a case. Our team can answer your questions and inform you of your legal options. You would pay nothing throughout the entire legal process unless we win your case.
Free Case Review | Available 24/7 | No Fee Until We Win
Phone (toll-free): 888-419-2229
Press the Live Chat button on your browser
Complete Our Online Contact Form
More about our firm
- About ABC Law Centers
- Meet our birth injury attorneys
- Meet our in-house medico-legal consultants
- Client testimonials
- Our awards
- Verdicts and settlements
More about pursuing a birth injury case
Video: the long-term effects of birth asphyxia
Watch a video of birth injury attorneys Jesse Reiter and Rebecca Walsh discussing the long-term effects of birth asphyxia. Birth asphyxia can often be prevented if the baby is quickly delivered at the first signs of distress. Failure to quickly deliver the baby can cause prolonged oxygen deprivation, hypoxic-ischemic encephalopathy (HIE), permanent brain damage, and conditions such as cerebral palsy.
Video: how is birth asphyxia pronounced?
Sources:
- (n.d.). Retrieved January 31, 2019, from https://www.uptodate.com/contents/systemic-effects-of-perinatal-asphyxia
- Ayres-de-Campos, D. (2017). Acute Fetal Hypoxia/Acidosis. In Obstetric Emergencies (pp. 7-25). Springer, Cham.
- Kang, S. K., & Kadam, S. D. (2015). Neonatal seizures: impact on neurodevelopmental outcomes. Frontiers in pediatrics, 3, 101.
- Gopagondanahalli, K. R., Li, J., Fahey, M. C., Hunt, R. W., Jenkin, G., Miller, S. L., & Malhotra, A. (2016). Preterm Hypoxic–ischemic encephalopathy. Frontiers in pediatrics, 4, 114.
- (n.d.). Retrieved January 31, 2019, from https://www.uptodate.com/contents/clinical-features-diagnosis-and-treatment-of-neonatal-encephalopathy
- Pasternak, J. F., & Gorey, M. T. (1998). The syndrome of acute near-total intrauterine asphyxia in the term infant. Pediatric neurology, 18(5), 391-398.
- Brain: Function and Anatomy of Parts, Diagram, Conditions, Health Tips. (n.d.). Retrieved January 31, 2019, from https://www.healthline.com/human-body-maps/brain#brain-diagram
- Cerebral Cortex. (n.d.). Retrieved January 31, 2019, from https://www.merriam-webster.com/dictionary/cerebral cortex
- Occipital Lobe Anatomy & Pictures | Body Maps. (n.d.). Retrieved January 31, 2019, from https://www.healthline.com/human-body-maps/occipital-lobe#1
- Cerebellum Function, Anatomy & Definition | Body Maps. (n.d.). Retrieved January 31, 2019, from https://www.healthline.com/human-body-maps/cerebellum#2
- Nicholls, J. G., & Paton, J. F. (2009). Brainstem: neural networks vital for life.




















