On the April 28th, 2006, Saynab Muse was admitted to the Ohio State University Medical Center at 3:20 p.m., already experiencing the initial stages of labor. From 3:20 until midnight, the fetal heart rate monitor showed a reassuring tracing. At midnight, the fetal monitor started showing abnormal tracings, with variable decelerations, which signal fetal distress that usually is related to oxygen deprivation. Despite poor fetal heart tracings, Pitocin was administered at 12:45 a.m. Intrauterine resuscitative measures were taken to address the decelerations between midnight and 3:00 a.m. This means that the 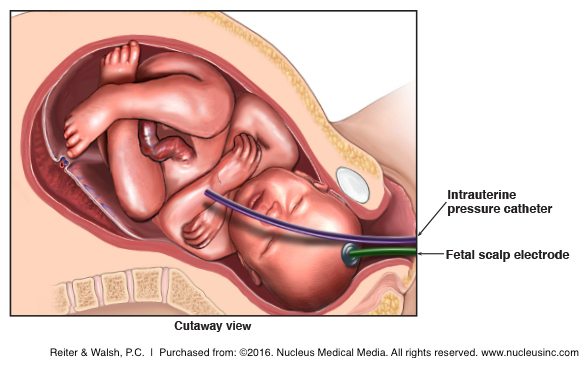 mother was given oxygen, fluids, amnioinfusion and position changes in order to increase oxygenation and perfusion (blood flow) to the placenta and umbilical cord, which would hopefully increase the oxygen-rich blood going to the baby. This was all an attempt to increase the baby’s oxygen level, which in turn would be reflected on the fetal heart monitor in the form of a reassuring heart tracing.
mother was given oxygen, fluids, amnioinfusion and position changes in order to increase oxygenation and perfusion (blood flow) to the placenta and umbilical cord, which would hopefully increase the oxygen-rich blood going to the baby. This was all an attempt to increase the baby’s oxygen level, which in turn would be reflected on the fetal heart monitor in the form of a reassuring heart tracing.
At 3:00 a.m., there was a prolonged deceleration in the fetal heart rate, despite the resuscitative measures. A prolonged deceleration is a decrease of 15 or more beats per minute below the baby’s baseline (baby’s heart rate pattern between contractions), and it usually signals a dangerous condition, and it always requires close attention. In fact, the deceleration lasted for 3 minutes, with a slow return to baseline. After that, the decelerations got progressively worse, and were occurring with almost every contraction. Between 0300 and 0400, there were very obvious decelerations, with beat to beat variability along with frequent uterine contractions.
A 2nd year resident had been taking care of the mother and baby after midnight, and even though the fetal heart tracing continued to be non-reassuring, the attending physician, Dr. Hull, was not called from the call room, where he was sleeping. In instances such as this, the standard of care requires that a physician with much more experience take over the care. An attending physician, such as Dr. Hull, should have been called. But Dr. Hull did not become involved until 0406. The standard of care also requires that steps be taken to address decelerations, and if the steps are unsuccessful, a C-section be ordered. In this case, a C-section should have been ordered no later than 04:10.* When fetal distress signs are present (signs that the baby is not being adequately oxygenated), the baby must be delivered before brain damage occurs.
When the various interventions performed between midnight and 0300 did not improve the fetal heart tracings – and in fact, the tracings got worse – something different should have been done. Standards of care allow obstetricians two options to ensure that the continuation of labor is safe for the baby. One option is to perform a test to make sure that the baby is not acidotic. (If a baby is acidotic, it means inadequate gas exchange is taking place and the baby is being deprived of oxygen.) If that test is not performed, the Pitocin must be stopped. One expert testified that had the Pitocin been stopped at 0300, the contractions would have spaced out, the decelerations would have stopped, and Ms. Muse would likely have delivered a healthy baby vaginally. However, if stopping the Pitocin did not improve the heart tracing, the standard of care required C-section delivery since vaginal delivery was not imminent. Even if the fetal acidosis test is not familiar to some obstetricians, all obstetricians are familiar with the necessity of calling a stat C-section when a fetal heart tracing does not improve despite resuscitative measures.
In Ms. Muse’s case, it is not as if there were just non-reassuring fetal heart tracings. The tracings were getting progressively worse, which was even more reason to stop Pitocin and perform a stat C-section. One of the experts stated that a fetus enduring all those decelerations despite intrauterine measures needs to be delivered immediately, because one never knows when the fetus will run out of reserves during labor. The expert explained that an obstetrician cannot wait until there is no variability (the heart tracing “flat lines”) to deliver the child. In this case, the baby was on the edge of a cliff, and if an obstetrician waits until no variability is seen, the baby is over the edge of the cliff, the expert further explained.
After hearing all the testimony, the court found that “the prolonged late decelerations would have alerted a physician of ordinary skill, care and diligence to closely monitor plaintiff for a period of time and re-examine her after 20 minutes to assess whether a c-section was warranted.”
“The evidence shows that at 4:10 a.m., the plaintiff was pushing poorly with contractions, and that when Dr. Hull performed an examination at 4:37 a.m., the baby’s head was in ‘minus one station,’ which means that delivery was not imminent,” according to the decision. “The court further finds that Dr. Hull’s delay in assessing the need for a c-section was the proximate cause of plaintiff’s injuries.”
The court found the testimony of the two plaintiffs’ expert witnesses “more persuasive.” Each physician found fault with how Pitocin was administered during labor.
One of the experts stated that Pitocin’s sole purpose “is to increase the frequency and intensity of uterine contractions, and in this case, the tracings showed that uterine contractions were causing decreased perfusion of blood and oxygen to the fetus.”
Another expert stated that “it was a breach of the standard of care to start the administration of Pitocin at 12:45 a.m., because plaintiff was experiencing increasing decelerations, and the Pitocin increased the amount of contractions which in turn decreased the amount of oxygen that was delivered to the baby.”
The baby, Ayub Gelle, suffered a “profound brain injury” as a result of the hypoxia and ischemia he experienced during labor. He is now 7 years old and requires around the clock care. Last week, OSU Medical Center agreed to pay Ms. Muse and her husband $5.25 million to help cover the lifelong care of Ayub. This is the second largest medical claim settled by OSU’s medical center.
IMPORTANCE OF QUICK AND APPROPRIATE RESPONSE TO NON-REASSURING FETAL HEART TRACINGS
This case underscores the importance of properly monitoring a baby during labor and responding appropriately to signs of fetal distress, such as non-reassuring tracings on the fetal monitor. The primary method of detecting fetal distress is through electronic fetal monitoring, which records both the mother’s contractions and the baby’s heart beat in response to contractions. Fetal distress almost always indicates that a baby is not receiving normal levels of oxygen.
It also is imperative for an obstetrician to be skilled in handling emergency situations that can arise during labor and delivery, especially if the physician creates a high risk situation for the mother and baby. In this case, the physicians administered Pitocin (oxytocin), which has been recognized as a dangerous drug. Pitocin increases the intensity and frequency of contractions, which can lead to hyperstimulation of the uterus. Hyperstimulation means the contractions are occurring so close together that there is almost no break in between them. When this occurs, the uterus is in a hypertonic state, or a state of almost constant contraction. Contraction causes the vessels in the placenta to be compressed, which means they cannot easily refill with fresh, oxygen-rich blood to be transported to the baby through the umbilical cord. This can cause the baby to be severely deprived of oxygen and can result in permanent brain damage, as was the case with baby Ayub.
Furthermore – and especially in the presence of non-reassuring heart tones and Pitocin use – a physician skilled and comfortable with emergency C-section delivery must be present during labor. When a baby shows signs of being oxygen deprived, the oxygen depriving conditions must either be removed, or the baby must be delivered immediately. Failure to follow standards of care and failure to act skillfully and quickly when a baby shows signs of distress constitute negligence. When this negligence causes injury in the baby, it is medical malpractice.
PITOCIN, FETAL MONITORING, DELAYED ACTION AND MEDICAL MALPRACTICE
If your labor was induced using Pitocin, or your physician failed to act appropriately and quickly to signs of fetal distress and your child has been diagnosed with permanent disabilities, call the nationally recognized birth injury attorneys at Reiter & Walsh ABC Law Centers: Birth Injury Lawyers. We will evaluate your child’s medical records and determine if negligence was the cause of your child’s injuries. Call us at 888-419-2229.
* In the plaintiff’s brief for this case, counsel states that the baby was suffering from hypoxia and ischemia long before 20 minutes before birth. However, the parties stipulated that the baby’s brain injury was the proximate result of hypoxia and ischemia during the last 15 – 20 minutes prior to delivery, which occurred at 5:10 a.m. Thus it was stipulated that the brain damage occurred between 0450 and 0510. This is the reason so much focus is placed on the latter part of delivery, even though standards of care were violated earlier in the labor.