Birth Injury
What is a birth injury?
A birth injury is any type of harm to a baby that occurs during or near the time of birth. This can include:
- oxygen deprivation (birth asphyxia)
- excessive pressure on the baby’s head or body (birth trauma)
- contracting an infection
- other complications
Although some birth injuries are very minor and leave no lasting impact, others can result in permanent disabilities, which may affect the child cognitively, emotionally, and/or physically.
In many cases, physicians can prevent birth injuries by following standards of care, carefully monitoring the health status of the mother and child, and promptly addressing any suspected issues that may arise during pregnancy, labor, and delivery. If a medical professional fails to do these things, and their negligence results in a birth injury, they have committed medical malpractice.

What are the most common types of birth injuries?
While there are many different types of birth injuries, some of the most common birth injuries include the following (3):
- Brachial plexus palsy: injury to a group of nerves that control arm and hand movement. It most often arises after a vaginal delivery with shoulder dystocia. The likelihood of complete recovery depends on the severity of the birth injury.
- Caput succedaneum:swelling of soft tissues in the baby’s scalp. It is more common in babies delivered with vacuum extraction. Caput succedaneum usually resolves without issue.
- Cephalohematoma: bleeding that occurs under a cranial bone. Usually, they go away within a few months, but serious cephalohematomas can lead to complications such as jaundice and can be a sign of more serious birth injuries.
- Clavicle or collarbone fractures: especially common in babies who were born breech or whose deliveries involved shoulder dystocia. Healing usually occurs quickly, but it may be necessary to limit the baby’s movement.
- Facial nerve palsy/paralysis, which may result from temporary nerve bruising. However, if it is due to a nerve tear, surgery may be needed to fix it.
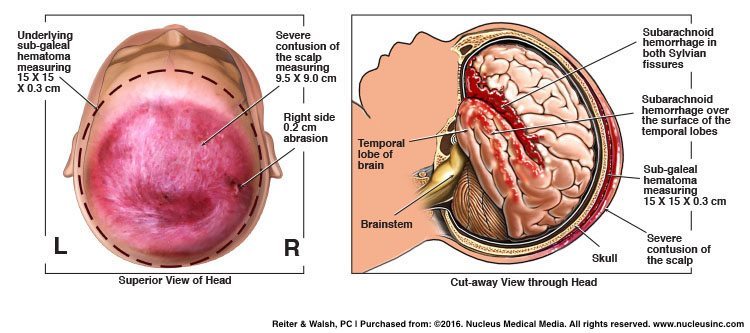
- Head trauma (bruising or lacerations) from passing through the birth canal and forceful contractions. The birth-assisting tools forceps and vacuum extractors can also cause head trauma. The severity of head trauma can vary greatly (see below).
- Hypoxic-ischemic encephalopathy (HIE): a type of brain damage caused by birth asphyxia (oxygen deprivation around the time of birth).
- Cerebral palsy (CP): can be caused by complications such as birth injury, birth asphyxia, birth trauma, and infection.
- Periventricular leukomalacia (PVL): damage to the brain’s white matter.
- Other types of brain damage, such as to the basal ganglia or cerebral cortex.
- Seizure disorders/epilepsy: can be caused by birth injuries such as HIE, birth trauma, or infection.
- Intellectual and developmental disabilities (I/DDs):often accompany other issues such as cerebral palsy or epilepsy.
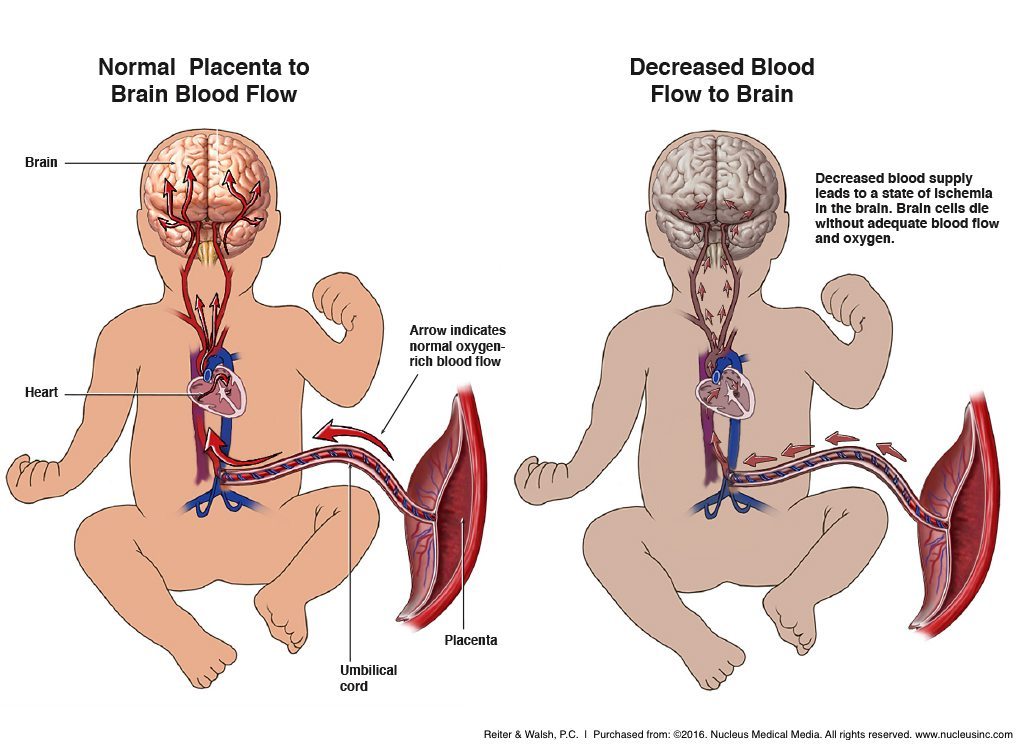
Birth injury caused by oxygen deprivation
Hypoxic-ischemic encephalopathy (HIE) & Birth Asphyxia
“Birth asphyxia” refers to oxygen deprivation around the time of birth, and hypoxic-ischemic encephalopathy (HIE) is brain damage that results from insufficient levels of oxygen and blood flowing to the infant’s brain. Babies with HIE also may have damage to other organs in addition to the brain, due to the spreading of cell death (4). In many cases, HIE is preventable with proper medical management. Moreover, after the initial injury occurs, permanent damage may be minimized if therapeutic hypothermia is administered very shortly after birth (5).
Obstetric complications that can cause HIE
The oxygen deprivation that leads to HIE can be caused by multiple factors, including (2):
- Umbilical cord problems such as cord prolapse, nuchal cord, short cord, and true knot.
- Uterine rupture, a complication in which the uterus tears, causing massive hemorrhage.
- Placental abruption, a complication in which the placenta separates from the uterine wall prior to the birth of the baby.
- Failure to quickly deliver the baby when oxygen deprivation (fetal distress) is evident on the heart rate monitor (see our page on delayed emergency C-section for more information).
Birth injury caused by trauma
Traumatic birth injuries are injuries caused by forces like pressure and torsion on the baby. Traumatic birth injuries can lead to other diagnoses such as HIE or cerebral palsy. When medical professionals adhere to standards of care, which include close monitoring of the mother and baby throughout pregnancy and delivery, traumatic birth can often be prevented. If a safe vaginal birth is unlikely (see below for some reasons why this may be the case), standard of care includes planning to deliver the baby via C-section. For less predictable complications, an emergency C-section may be necessary.
Obstetric events that can cause traumatic birth
Traumatic birth can be caused by multiple factors, including (3):
- An abnormal fetal presentation, such as face or breech presentation. This can make delivery difficult and cause trauma to the baby’s head and/or neck.
- Improper use of vacuum extractors or forceps. This can put pressure on the baby’s delicate skull and brain, collapsing fragile blood vessels and causing HIE.
- Situations in which the baby is ‘stuck’ in the birth canal due to a size mismatch between the mother’s pelvis and the baby’s head (cephalopelvic disproportion) or because the baby is much larger than average for their gestational age (macrosomia).
- Prolonged or arrested labor, wherein the baby either moves too slowly down the birth canal or doesn’t progress down the canal. The contractions of labor place pressure on the baby’s head. Consequently, exposure to contractions for too long can cause the head to be compressed, which in turn can compromise blood flow to certain parts of the brain.
Birth injury and prematurity
Babies who are born prematurely are not yet fully developed. Their brains, lungs, and other organs still have not yet fully matured, which means that they are more susceptible to birth injury and may require medical interventions for neonatal breathing problems (6).
They often go to the NICU, where they may be placed on breathing machines. It is very important that the breathing machines be properly regulated, because if they are not, they may drive down the amount of carbon dioxide in the baby’s blood to dangerous levels.
This overventilation can lead to brain damage and tissue loss, such as periventricular leukomalacia (PVL). The signs of PVL are not always immediately apparent, but can put babies at risk for complications such as motor disorders, cognitive impairments, seizures, and vision and hearing problems.
Medical staff should screen for risk factors that can cause or contribute to premature birth in order to provide interventions that can prevent premature birth.
Birth injury stemming from improper NICU care
Many of the aforementioned injuries may result in a baby needing treatment in the Neonatal Intensive Care Unit (NICU). However, improper NICU care can cause further injury.
It is very important to keep babies in the NICU properly fed, especially if they have neonatal hypoglycemia (low blood sugar). Glucose is the brain’s only source of energy, and if a baby’s blood sugar drops too low, this can cause brain injury.
Many babies in the NICU have jaundice. Jaundice is a medical condition in which bilirubin (a byproduct of blood cells) builds up in the tissues, causing the skin and/or eyes to look yellowed. In some cases, jaundice goes away on its own.
In other cases, a baby may need help getting rid of the extra bilirubin. They can be put under blue phototherapy lights, which help the body get rid of the bilirubin safely. If too much bilirubin builds up in the baby’s body, it can cross through the blood-brain barrier and cause a form of brain damage known as kernicterus. Kernicterus is always preventable with proper medical treatment for jaundice.
Birth injury caused by improper prenatal care
It is very important that prenatal care be thorough, including frequent ultrasounds and other testing. Medical providers should provide tests to help recognize potential risk factors for birth injury, such as umbilical cord problems, issues with fetal growth (IUGR), or maternal medical conditions (discussed later). If these issues are identified early, birth injuries can often be prevented.
Birth injury caused by infection
During labor and delivery, babies are in contact with the mother’s birth canal, which means they are exposed to the mother’s bacteria and viruses. Many bacterial and viral strains are harmless, but not all.
Medical professionals should run tests for certain kinds of maternal infections during prenatal care. If these infections are not properly identified and treated (with antibiotics or antivirals), they can travel to and infect the baby’s brain (encephalitis), the membranes surrounding the brain and spinal cord (meningitis), or the lungs (pneumonia). Click here to learn more about neonatal infections.
Birth injury caused by untreated or mistreated maternal medical conditions (high-risk pregnancy)
In addition to infections, there are many other maternal health conditions that can increase the risk of birth injury to the baby. These conditions can make a pregnancy ‘high-risk,’ which means that the mother and baby may need additional monitoring and interventions to prevent birth injury. Some examples of high-risk pregnancy conditions include the following (7):
- Diabetes and gestational diabetes
- Oligohydramnios
- Post-term pregnancy
- High blood pressure and preeclampsia
- Premature rupture of membranes (PROM)
- Obesity
- Multiples (twins, triplets or more)
- Advanced maternal age (over 35)
- Other health conditions (such as PCOS, kidney disease, autoimmune disorders, thyroid issues, or HIV/AIDS)
With high-risk pregnancies, prenatal care visits are often more frequent and involve more tests to ensure that both mother and baby are progressing well through the pregnancy. For the baby, tests (such as NSTs and BPPs) may be done to ensure they are getting enough blood flow, oxygen, and nutrients. In some circumstances, an early planned delivery may be recommended, especially in cases where certain infections, high blood pressure issues, or diabetes are a factor in the mother’s pregnancy.
Birth injury caused by mismanaged obstetric procedures and emergencies
Labor and delivery can rapidly change from normal conditions to those that require prompt or emergency intervention. Medical staff should be properly trained and have experience in handling obstetric emergencies.
Situations that can quickly become obstetric emergencies include:
- Fetal distress (fetal oxygen deprivation, which shows up as non-reassuring tracings on fetal monitoring strips)
- Umbilical cord prolapse (where the umbilical cord descends in front of or alongside the baby, becoming compressed between the baby’s presenting part and the birth canal)
- Uterine rupture (where the uterus tears, causing massive hemorrhage)
- Placental abruption (where the placenta separates prematurely from the uterine wall, causing bleeding)
- Labor in the presence of placenta previa (a low-lying placenta, which either completely or fully covers the cervix)
- Vaginal Birth after C-Section (VBAC): Women with prior C-section scars have an increased risk of abdominal rupture if they undergo labor after their C-section.
- Neonatal Resuscitation: After delivery, babies that aren’t breathing at birth, or are struggling to breathe, need emergency resuscitation. If resuscitation is done incorrectly, this can injure the baby by damaging the lungs.
Other situations and delivery room errors that increase the risk of birth injury include:
- Delayed delivery: When medical staff waits too long to induce or deliver a baby, it can cause birth injury. Medical staff should be trained to recognize situations in which a prompt delivery is necessary, including fetal distress and other obstetric emergencies. The longer medical staff allow labor to progress on in the presence of these emergencies, the greater the risk of birth injury. No more than 30 minutes should elapse between the decision to have an emergency C-section and incision time.
- Improper fetal monitoring: Babies’ heart rates should be continuously monitored during labor and delivery to ensure they tolerate labor well. If fetal monitoring is done improperly, medical staff may miss signs of fetal distress, missing a critical window of time to intervene to prevent a birth injury.
- Improper anesthesia administration: While many individuals choose to use an epidural during labor, it is important to note that epidurals do carry risks. If improperly administered, they can interfere with the second stage of labor and cause low blood pressure in the mother, which can, in turn, impact blood flow to the baby. In some cases, anesthesia may interfere with bearing-down, which increases the chances that drugs like pitocin or cytotec may be used to augment labor.
- Improper pitocin or : Pitocin and cytotec are often used to augment contractions. However, in some situations, they may make contractions too strong (uterine tachysystole), and reduce blood flow to the baby.
Birth injury treatment
Birth injuries can cause permanent brain damage. Once this permanent brain damage occurs, much of the care available is supportive and palliative, with the exception of hypothermia therapy to reduce the severity of injury for hypoxic-ischemic encephalopathy (HIE). Hypothermia therapy should be given within the first six hours of birth.
For any baby that has been birth-injured, the medical team must carefully monitor their health and prevent further harm from complications such as seizures, poor perfusion, imbalances of electrolytes and blood sugar, brain bleeds, respiratory problems, and infections.
Moreover, babies with birth injuries are often enrolled in Early Intervention (EI) programs and provided with numerous therapies to help them maximize their skills and development. These include physical therapy (to help with gross motor skills), occupational therapy (to help with fine motor skills), speech therapy (to help with communication and/or swallowing difficulties), and other therapies as needed.
The information presented above is intended only to be a general educational resource. It is not intended to be (and should not be interpreted as) medical advice.


Attorneys helping children with HIE, cerebral palsy, and other birth injuries
At ABC Law Centers: Birth Injury Lawyers (Reiter & Walsh, P.C.), we focus solely on birth injury. We have been advocating for children since our inception in 1997. Our Michigan-based attorneys and in-house medical staff have helped families throughout the country obtain compensation for lifelong treatment, therapy, and a secure future.
We can also handle FTCA cases involving military medical malpractice and federally-funded clinics.
Contact us to begin your free case evaluation. Our award-winning birth injury lawyers are available 24/7 to speak with you.



Featured Videos
Posterior Position
Hypoxic-Ischemic Encephalopathy (HIE)

Featured Testimonial
What Our
Clients Say…
After the traumatic birth of my son, I was left confused, afraid, and seeking answers. We needed someone we could trust and depend on. ABC Law Centers: Birth Injury Lawyers was just that.
- Michael
Helpful resources
- Reiter, J. (2014, November 14). How Can I Tell If My Child Has Cerebral Palsy? Retrieved May 13, 2020, from https://www.abclawcenters.com/frequently-asked-questions/how-can-i-tell-if-my-child-has-cerebral-palsy/
- Hypoxic-Ischemic Encephalopathy (HIE): Legal Help for Birth Injuries. (n.d.). Retrieved May 13, 2020, from https://www.abclawcenters.com/practice-areas/prenatal-birth-injuries/fetus-or-newborn-medical-problems/hypoxic-ischemic-encephalopathy/#signs
- Default – Stanford Children’s Health. (n.d.). Retrieved from https://www.stanfordchildrens.org/en/topic/default?id=birth-injury-90-P02340
- Hypoxic-Ischemic Encephalopathy: Practice Essentials, Background, Pathophysiology. (2018, July 26). Retrieved from https://emedicine.medscape.com/article/973501-overview
- Laptook, A. R., Shankaran, S., Tyson, J. E., Munoz, B., Bell, E. F., Goldberg, R. N., … & Das, A. (2017). Effect of therapeutic hypothermia initiated after 6 hours of age on death or disability among newborns with hypoxic-ischemic encephalopathy: A randomized clinical trial. Jama, 318(16), 1550-1560.
- Premature birth. (2017, December 21). Retrieved May 13, 2020, from https://www.mayoclinic.org/diseases-conditions/premature-birth/symptoms-causes/syc-20376730
- Reiter, J. (2014, November 14). Medical Mistakes and Birth Injury: FAQs. Retrieved May 13, 2020, from https://www.abclawcenters.com/frequently-asked-questions/what-is-a-high-risk-pregnancy/