What is premature rupture of the membranes (PROM), and how can it be prevented?
Premature Rupture of the Membranes (PROM) is a complication occurring during pregnancy in which the mother’s membranes rupture (this is commonly referred to as the “water breaking”) more than an hour before labor begins. PROM puts unborn babies at risk of not getting enough oxygen because their umbilical cord becomes compressed, as well as becoming infected and experiencing other dangerous consequences. Prolonged PROM is when PROM happens more than 18 hours before labor. Preterm PROM (PPROM) is when PROM happens before the baby is at 37 weeks of gestation. All these conditions can put the baby at risk of birth injuries, and sometimes lead to permanent disabilities such as hypoxic-ischemic encephalopathy (HIE) and cerebral palsy (CP). However, when medical professionals properly manage deliveries involving PROM, harm can be avoided.
Causes And Risk Factors For Premature Rupture Of The Membranes (PROM)
Circumstances that can cause or increase the risk of PROM include the following:
- The mother had prior preterm PROM (PPROM)
- The mother had prior preterm labor and delivery
- The mother has an infection, such as herpes simplex virus (HSV), Group B Strep (GBS), bacterial vaginosis (BV), or a urinary tract infection (UTI)
- Chorioamnionitis is present
- The mother is experiencing bleeding from the vagina
- The mother smokes
- The mother has poor nutrition
- The mother has had previous cervical surgery, including cone biopsies or cerclage
- The mother has had overstretching of her uterus and amniotic sac, which sometimes occurs with multiple fetuses (past or current twin or triplet pregnancies) or too much amniotic fluid (polyhydramnios)
- The mother has sepsis (inflammation and infection in the entire body)
- Umbilical cord prolapse
- Malpresentation of the baby, such as face or breech presentation
- Cervical incompetence or insufficiency
- Shortening of the cervix
Signs And Symptoms Of Premature Rupture Of The Membranes (PROM)
The most significant sign of PROM is fluid leaking from the vagina. When the mother’s water breaks, it may feel like a slow trickle of fluid from the vagina or a sudden gush of fluid that is pale yellow or clear.
PROM and infection often occur together. It therefore is crucial to recognize the signs of infection in a pregnant woman. Signs of maternal infection include the following:
- An increase in the fetal heart rate
- Contractions of the uterus (womb)
- Increased heart rate and temperature in the mother
- Tenderness of the uterus
- Bad smelling vaginal discharge
- Increased white blood cell count or a change in the pattern of white blood cell type in the mother
Diagnosing Premature Rupture Of The Membranes (PROM)
Physicians diagnose PROM by using a speculum to determine if fluid is leaking from the cervix. A sample of fluid from the vagina is examined under a microscope and tested with special paper to verify that the fluid is amniotic. An ultrasound also may be used to determine the amount of amniotic fluid around the baby. In addition to these tests, a crucial part of diagnosing PROM involves taking a thorough history of the mother. The physician must ask appropriate questions to determine if the mother has signs and symptoms of PROM, as well as risk factors for the condition.
Complications And Injuries Associated With Premature Rupture Of The Membranes
Complications associated with PROM include:
- Chorioamnionitis: Chorioamnionitis is inflammation and infection of the placenta and fetal membranes, caused by bacteria ascending into the uterus from the vagina or occasionally the colon.
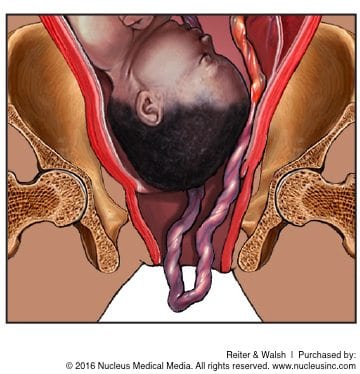
Umbilical cord compression: After a premature rupture of membranes, the umbilical cord is no longer cushioned by the amniotic fluid, and can become compressed (or flattened). In some cases, the umbilical cord may also slip out of the birth canal in front of the baby, becoming compressed between the presenting part of the baby (usually the head) and the mother’s vaginal canal. This is known as cord prolapse. Cord prolapse and other forms of compression are dangerous because the flow of oxygen-rich blood to the baby is interrupted, and the baby may experience dangerous complications like HIE. - Maternal infection: Without the protection of the amniotic sac, maternal infections can be easily transmitted to the baby, potential leading to sepsis, meningitis, and permanent brain damage.
- Death of the baby
- Overventilation injuries: Overventilation injuries can occur when babies are put on breathing machines and are not closely monitored.
Treatment For Premature Rupture Of The Membranes (PROM)
Treatment for PROM at Term
In a term pregnancy where PROM has occurred, allowing labor to occur spontaneously is often the standard of care. The standard includes induction of labor at approximately 12 hours if it has not already begun. Some physicians induce labor immediately, but prevention of Group B Strep (GBS) transmission to the baby must be considered. If the GBS status of the mother is unknown, the physician should typically administer antibiotics so that if the mother has GBS, the infection will not be transmitted to the baby. Research suggests that a mother who has labor induced by the physician is less likely to develop an infection in her uterus (womb) than a mother who waits for labor to start naturally. Of course, when infection is present, antibiotics must always be given.
Treatment for Preterm Premature Rupture of Membranes (PPROM)
When membranes rupture between weeks 34 and 37 of pregnancy, standard of care is similar to that for at-term PROM. In most cases, the physician should induce labor. The thinking behind this is that the risk of infection and complications associated with infection outweigh the risks associated with the baby being born a few weeks early.
If the membranes rupture before 34 weeks of gestation, the situation is much more complex. If there are no signs of infection, the physician may try to delay labor with medication (such as terbutaline and brethine) until the baby’s lungs are more mature. Antibiotics should typically be given, and steroids (such as betamethasone) may be administered to help the baby’s lungs mature more quickly and to provide neuroprotective benefits. In some cases, a sample of amniotic fluid may be collected to determine the baby’s lung maturity. If the baby’s lungs are mature, labor will usually be induced.
When membranes rupture between weeks 32 and 34, careful evaluation and close monitoring is required.
When membranes rupture before 32 weeks of gestation, an attempt is usually made to delay delivery. A course of steroids should be given for fetal lung maturity. Research shows that the incidence of neonatal death, respiratory distress syndrome (RDS), and intraventricular hemorrhages (brain bleeds) is significantly decreased when the baby receives steroids in the womb at this age. In addition, the length of time a newborn has to be on a breathing machine is greatly reduced. Babies delivered at 32 weeks or earlier often have RDS and intraventricular hemorrhages (IVH), and therefore need to be very closely monitored.
It is crucial to understand that that a premature baby with an infection is at higher risk than an uninfected premature baby. Ideally, the baby should be delivered before the uterus and baby become infected. The timing of this is sometimes difficult to predict, so close monitoring is essential, and signs of infection or changes in the baby’s testing (even subtle ones) should be relied upon.
Antibiotics For Prevention Of Infection After Premature Rupture Of The Membranes (PROM)
Antibiotics should be administered because infection may be both a cause and consequence of PROM, and it is related to preterm delivery. The goal of antibiotic therapy is to decrease the frequency of maternal and fetal infection and delay the onset of preterm labor, and to minimize the risk of chorioamnionitis, cerebral palsy, and other known complications associated with infection.
C-Section Delivery And Premature Rupture Of The Membranes (PROM)
Risk of infection increases with the amount of time that passes between the rupture of membranes and the delivery of the baby. The risk greatly increases if labor does not occur within 12 hours of the membranes rupturing. The main goal is to keep the baby safe, so it is crucial to protect a baby from infection. It is also critical to protect the baby from the injuries and complications that may occur if physicians wait for the delivery to begin naturally. Delaying delivery could lead to utilization of forceps and vacuum extractors which carry the risk of traumatic birth injuries to the delicate baby, or administering potentially dangerous drugs like Cytotec and Pitocin to speed up delivery. Many times, an emergent cesarean section is needed to protect the health of the baby.
Premature Rupture Of The Membranes (PROM) And Umbilical Cord Compression
Umbilical cord compression is a serious complication associated with PROM. If the baby’s heart rate drops below 100 for 60 seconds or more, there is a significant chance the cord is compressed. Very close monitoring is crucial at this point, and if the cord is compressed, delivery must occur right away. Mismanaged umbilical cord compression can lead to hypoxic-ischemic encephalopathy (HIE; birth asphyxia), infant brain damage, cerebral palsy, and other permanent injuries and disabilities.
Rupture of the Membranes and Medical Malpractice

Babies born after PROM occurs typically do well, as long as their conditions are properly managed and standards of care are followed. This means that infection must be avoided, umbilical cord compression must be promptly addressed, and complications associated with breathing problems should be prevented. Steroids can be given in utero to help a baby’s lungs mature, and if the lungs are immature after birth, the baby can be given surfactant. It is critical for physicians to closely monitor the baby for any breathing issues. This requires a lot of skill, as well as consultation with specialists. If a baby is having trouble breathing, treatment (including placing the baby on a breathing machine) should be implemented. There are many different types of breathing machines that can be used to help a baby breathe, and when skillfully used, the baby can be gently and safely ventilated. It is critical to closely watch a baby on a breathing machine so that overventilation complications can be avoided.
All issues involved with a baby born following PROM require careful consideration and skill. If a physician or medical team fail to follow medical guidelines and standards of care, properly monitor the infant, or perform a timely C-section when necessary, it is negligence. If this negligence leads to injury of the mother or baby, it is medical malpractice.
Legal Help for Birth Injuries from Premature Rupture of the Membranes (PROM)
If you experienced PROM and your baby was diagnosed with a birth injury such as hypoxic-ischemic encephalopathy (HIE), cerebral palsy (CP), or intellectual and developmental disabilities, the award-winning attorneys at Reiter & Walsh ABC Law Centers: Birth Injury Lawyers can help. Our legal team has helped children throughout the country obtain compensation for lifelong treatment, therapy, and a secure future, and we give personal attention to each child and family we represent. Because we exclusively focus on birth injury cases, our attorneys have decades of joint experience specifically handling the complications and medical errors responsible for your loved one’s injuries. Our firm has numerous multi-million dollar verdicts and settlements that attest to our success, and you pay nothing until we win your case.
Free Case Review | Available 24/7 | No Fee Until We Win
Call our toll-free phone line at 888-419-2229
Press the Live Chat button on your browser
Complete Our Online Contact Form